Homeostasis and gas exchange.

Gas exchange.
Homeostasis is maintained by the respiratory system in two ways: gas exchange and regulation of blood pH. Gas exchange is performed by the lungs by eliminating carbon dioxide, a waste product given off by cellular respiration. As carbon dioxide exits the body, oxygen needed for cellular respiration enters the body through the lungs. ATP, produced by cellular respiration, provides the energy for the body to perform many functions, including nerve conduction and muscle contraction. Lack of oxygen affects brain function, sense of judgment, and a host of other problems.
Gas exchange.
Gas exchange in the lungs and in the alveoli is between the alveolar air and the blood in the pulmonary capillaries. This exchange is a result of increased concentration of oxygen, and a decrease of C02. This process of exchange is done through diffusion.
External respiration.
External respiration is the exchange of gas between the air in the alveoli and the blood within the pulmonary capillaries. A normal rate of respiration is 12-25 breaths per minute. In external respiration, gases diffuse in either direction across the walls of the alveoli. Oxygen diffuses from the air into the blood and carbon dioxide diffuses out of the blood into the air. Most of the carbon dioxide is carried to the lungs in plasma as bicarbonate ions (HCO3-). When blood enters the pulmonary capillaries, the bicarbonate ions and hydrogen ions are converted to carbonic acid (H2CO3) and then back into carbon dioxide (CO2) and water. This chemical reaction also uses up hydrogen ions. The removal of these ions gives the blood a more neutral pH, allowing hemoglobin to bind up more oxygen. De-oxygenated blood "blue blood" coming from the pulmonary arteries, generally has an oxygen partial pressure (pp) of 40 mmHg and CO2 pp of 45 mmHg. Oxygenated blood leaving the lungs via the pulmonary veins has a O2 pp of 100 mmHg and CO2 pp of 40 mmHg. It should be noted that alveolar O2 pp is 105 mmHg, and not 100 mmHg. The reason why pulmonary venous return blood has a lower than expected O2 pp can be explained by "Ventilation Perfusion Mismatch".
Internal respiration.
Internal respiration is the exchanging of gases at the cellular level.
The passage way from the trachea to the bronchioles.
There is a point at the inferior portion of the trachea where it branches into two directions that form the right and left primary bronchus. This point is called the Carina which is the keel-like cartilage plate at the division point. We are now at the Bronchial Tree. It is named so because it has a series of respiratory tubes that branch off into smaller and smaller tubes as they run throughout the lungs.
Right and left lungs.
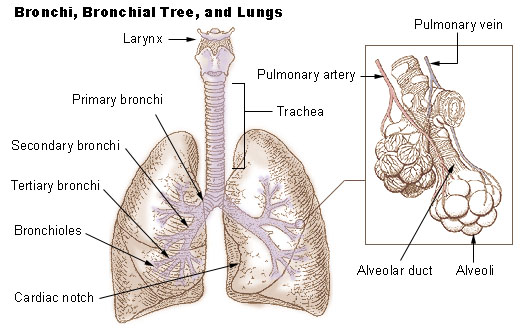
Diagram of the lungs.
The right primary bronchus is the first portion we come to, it then branches off into the lobar (secondary) bronchi, segmental (tertiary) bronchi, then to the Bronchioles which have little cartilage and are lined by simple cuboidal epithelium (See fig. 1). The bronchi are lined by pseudostratified columnar epithelium. Objects will likely lodge here at the junction of the Carina and the Right Primary Bronchus because of the vertical structure. Items have a tendency to fall in it, where as the Left Primary Bronchus has more of a curve to it which would make it hard to have things lodge there.
The left primary bronchus has the same setup as the right with the lobar, segmental bronchi and the bronchioles.
The lungs are attached to the heart and trachea through structures that are called the roots of the lungs. The roots of the lungs are the bronchi, pulmonary vessels, bronchial vessels, lymphatic vessels, and nerves. These structures enter and leave at the hilus of the lung which is "the depression in the medial surface of a lung that forms the opening through which the bronchus, blood vessels, and nerves pass" (medlineplus.gov).
There are a number of terminal bronchioles connected to respiratory bronchioles which then advance into the alveolar ducts that then become alveolar sacs. Each bronchiole terminates in an elongated space enclosed by many air sacs called alveoli which are surrounded by blood capillaries. Present there as well, are Alveolar macrophages, they ingest any microbes that reach the alveoli. The pulmonary alveoli are microscopic, which means they can only be seen through a microscope, membranous air sacs within the lungs. They are units of respiration and the site of gas exchange between the respiratory and circulatory systems.
Cellular respiration.
First the oxygen must diffuse from the alveolus into the capillaries. It is able to do this because the capillaries are permeable to oxygen. After it is in the capillary, about 5% will be dissolved in the blood plasma. The other oxygen will bind to red blood cells. The red blood cells contain hemoglobin that carries oxygen. Blood with hemoglobin is able to transport 26 times more oxygen than plasma without hemoglobin. Our bodies would have to work much harder pumping more blood to supply our cells with oxygen without the help of hemoglobin. Once it diffuses by osmosis it combines with the hemoglobin to form oxyhemoglobin.
Now the blood carrying oxygen is pumped through the heart to the rest of the body. Oxygen will travel in the blood into arteries, arterioles, and eventually capillaries where it will be very close to body cells. Now with different conditions in temperature and pH (warmer and more acidic than in the lungs), and with pressure being exerted on the cells, the hemoglobin will give up the oxygen where it will diffuse to the cells to be used for cellular respiration, also called aerobic respiration. Cellular respiration is the process of moving energy from one chemical form (glucose) into another (ATP), since all cells use ATP for all metabolic reactions.
It is in the mitochondria of the cells where oxygen is actually consumed and carbon dioxide produced. Oxygen is produced as it combines with hydrogen ions to form water at the end of the electron transport chain (see chapter on cells). As cells take apart the carbon molecules from glucose, these get released as carbon dioxide. Each body cell releases carbon dioxide into nearby capillaries by diffusion, because the level of carbon dioxide is higher in the body cells than in the blood. In the capillaries, some of the carbon dioxide is dissolved in plasma and some is taken by the hemoglobin, but most enters the red blood cells where it binds with water to form carbonic acid. It travels to the capillaries surrounding the lung where a water molecule leaves, causing it to turn back into carbon dioxide. It then enters the lungs where it is exhaled into the atmosphere.
Lung capacity.
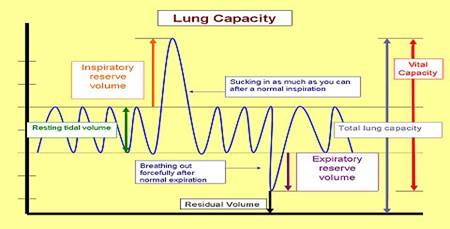
The normal volume moved in or out of the lungs during quiet breathing is called tidal volume. When we are in a relaxed state, only a small amount of air is brought in and out, about 500 mL. You can increase both the amount you inhale, and the amount you exhale, by breathing deeply. Breathing in very deeply is Inspiratory reserve volume and can increase lung volume by 2900 mL, which is quite a bit more than the tidal volume of 500 mL. We can also increase expiration by contracting our thoracic and abdominal muscles. This is called expiratory reserve volume and is about 1400 ml of air. Vital capacity is the total of tidal, inspiratory reserve and expiratory reserve volumes; it is called vital capacity because it is vital for life, and the more air you can move, the better off you are. There are a number of illnesses that we will discuss later in the chapter that decrease vital capacity. Vital Capacity can vary a little depending on how much we can increase inspiration by expanding our chest and lungs. Some air that we breathe never even reaches the lungs! Instead it fills our nasal cavities, trachea, bronchi, and bronchioles. These passages aren't used in gas exchange so they are considered to be dead air space. To make sure that the inhaled air gets to the lungs, we need to breathe slowly and deeply. Even when we exhale deeply some air is still in the lungs,(about 1000 ml) and is called residual volume. This air isn't useful for gas exchange. There are certain types of diseases of the lung where residual volume builds up because the person cannot fully empty the lungs. This means that the vital capacity is also reduced because their lungs are filled with useless air.